Clinical History
None Available.


Diagnosis:
Adrenal Myelolipoma
What is the most common presentation of these lesions?
- Asymptomatic
- Flank pain
- Endocrine disturbance
- Distant metastases
Answer: These patients are usually asymptomatic.
Regarding adrenal myelolipomas (please select True or False):
- T or F: Most myelolipomas are bilateral.
- T or F: Most myelolipomas are found as an incidental finding on imaging for another purpose.
- T or F: Myelolipomas are at risk for malignant transformation.
- T or F: Biopsy is often necessary to confirm diagnosis.
- T or F: Myelolipomas may hemorrhage.
Answers: F,T, F, F, T
Case Points:
- Adrenal myelolipoma is a benign neoplasm comprised of mature adipocytes and varying amounts of hematopoietic elements.
- Myelolipomas are most often an incidental finding and are not at risk for malignant degeneration.
Discussion:
Myelolipomas are rare benign neoplasms of uncertain etiology; however, the most accepted pathophysiology is that of adrenal cortical metaplasia with degeneration secondary to chronic stress or chronic illness. These tumors are most commonly diagnosed incidentally at imaging or at autopsy and can vary in size from sub-cm up to 30cm. Myelipomas are nonfunctioning tumors, and most patients are asymptomatic; however, hemorrhage into the tumor can cause flank pain.
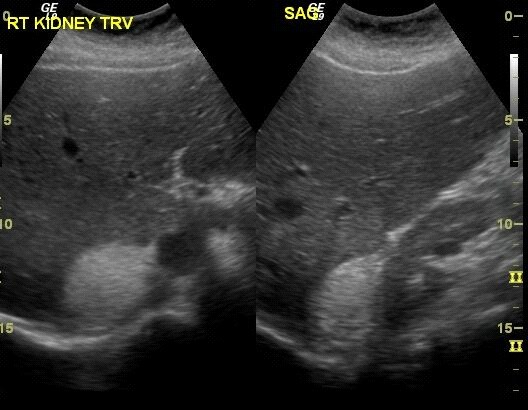
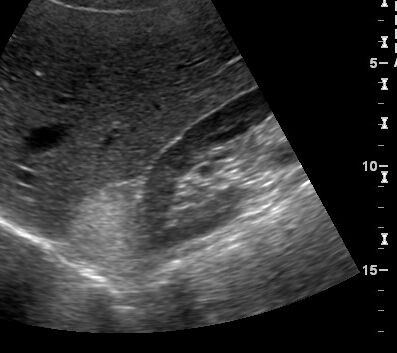
Classic imaging findings on US, CT, and MR allow for a presumptive diagnosis in most cases. At sonography, a suprarenal lesion is seen with a heterogeneous appearance containing echogenic and hypoechoic foci; these correlate with fatty elements and hematopoietic elements, respectively. Calcification can be associated with these lesions which will be seen as shadowing foci within the mass. At CT, myeloplipomas will contain a percentage of fat interspersed with low attenuation hematopoietic elements. These elements are often mistakenly described as soft tissue attenuation foci; however, the hematopoetic elements classically measure between 20-30 HU. Likewise at MR, T1 hyperintensity correlates with the fat containing areas which will appropriately drop out after fat saturation. The marrow containing elements are more classically isointense to spleen. No further work-up is needed after a fat containing adrenal lesion is characterized on CT or MR.
Asymptomatic patients do not require treatment for these lesions. If the lesion enlarges or undergoes hemorrhage, surgical excision can be performed. Extraadrenal myelolipomas are rare and only account for less that 15% of myelolipomas. The most common location for extraadrenal myelolipomas is within the retroperitoneum followed by the chest. Imaging characteristics for these tumors are the same as for typical adrenal myelolipomas.
Melany Atkins, M.D.
Department of Radiology, University of Pittsburgh School of Medicine
References:
- Rao, P. MD. Kenney, P. MD. Wagner, B. MD. Davidson, A., MD. Imaging and Pathologic Features of Myelolipoma. Radiographics 1997; 17:1373.
- Han, M. Burnett, A. Fishman, E. Marshall, F. The natural history and Treatment of Adrenal Myelolipoma. The journal of Urology. 1997. 157:1213.
- Carroll, B. Ultrasound case of the day. Myelolipoma of the right adrenal gland. Radiographics. 1991. 11:927.
- Otal, P. Escourrou, G. Maxerolles, C. D’Othee, B. Mezghani, S. Musso, S. Colombier, D. Rousseau, H. Joffre, F. Imaging Features of Uncommon Adrenal Masses with Histopathologic Correlation. Radiographics. 1999. 19:569.