Clinical history:
33 yo F presents to the ED with pelvic pain. Patient is 7 weeks pregnant by history.

This image shows an empty endometrial cavity with a fibroid that partially obscures and displaces the endometrial cavity. No intrauterine pregnancy is identified on this image.
Question 1: True or False? The absence of an intrauterine pregnancy in the presence of a positive pregnancy test is diagnostic of an ectopic pregnancy.

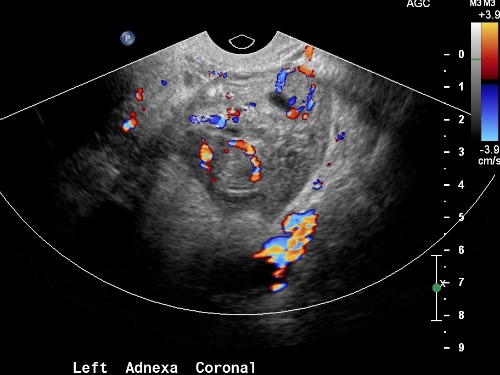
These images demonstrates a mass in the region of the ovary. It is unclear based on this image alone whether the mass is intrinsic or extrinsic to the ovary. Color Doppler demonstrates two “rings of fire.”

Normal right ovary.
Question 2: True or False? Corpus luteum cysts in the ovary can mimic paraovarian ectopic pregnancy.
This cine (video) clip demonstrates separate movement of the adnexal mass from the ovary using real time visualization of the ovary during compression with the ultrasound probe.
Question 3: What finding is seen in the images to suggest the diagnosis of ectopic pregnancy over corpus luteal cyst?
- Separation of the mass from the ovary with compression
- Ring of fire pattern of Doppler flow
- Demonstration of an embryo within the gestational sac
- Free fluid in the pelvis
Answers:
Question 1: False. The differential diagnosis for this situation is: spontaneous abortion, early intrauterine pregnancy, and ectopic pregnancy.
Question 2: True.
Question 3: A.
Discussion:
When a patient presents with a positive pregnancy test and an ultrasound that fails to demonstrate an intrauterine pregnancy, the differential diagnosis includes spontaneous abortion, early intrauterine pregnancy (too small to see with ultrasound), and ectopic pregnancy. Features that may suggest spontaneous abortion include: history of vaginal bleeding, endometrial thickening, and/or heterogeneous contents in the endometrial cavity. Features suggestive of early intrauterine pregnancy include a low quantitative beta-hCG, and no extra-uterine mass. Ectopic pregnancy is an important diagnosis to make to avoid morbidity and mortality. The majority of ectopic pregnancies occur in the fallopian tubes. Tubal ectopic pregnancy is diagnosed by using ultrasound to visualize an adnexal mass separate from the ovary. When an ectopic pregnancy occurs adjacent to the ovary, it is often difficult to differentiate an ectopic pregnancy from a corpus luteal cyst in the ovary.
There are several features of that have been suggested to help distinguish ectopic pregnancy from corpus luteal cyst. Because medical or surgical interventions are indicated for ectopic pregnancy vs. observation for corpus luteal cyst, distinguishing the two is important in the management of the patient. High resistive index may be more suggestive of ectopic pregnancy; however there is a fair amount of variation in the RI in both ectopic pregnancy and corpus luteal cyst. The echogenicity of the wall of the ectopic pregnancy will may be increased compared to the endometrium and a corpus luteal cyst may be isoechoic or hypoechoic when compared with the endometrium. The internal echo patterns have also been studied. The only internal echo pattern than has some utility in differentiating the two diagnoses is an anechoic appearance, which tends to be more predictive of corpus luteal cyst. Free fluid in the pelvis, suggestive of hemoperitoneum, can sometimes be helpful in diagnosing ectopic pregnancy, but can also be seen in ruptured hemorrhagic cyst. Doppler has been less useful because both ectopic pregnancy and corpus luteal cyst can have a similar “ring of fire” appearance.
A 2005 study in the Journal of Ultrasound in Medicine found that independent movement of a paraovarian mass from the ovary with ultrasound compression had negative and positive predictive values of 96.1% and 77.8% respectively. The sensitivity and specificity for mass separation with compression were 89.1% and 91.3% respectively. Mass separation with compression was the finding that was used in this case to distinguish ectopic pregnancy from corpus luteal cyst.
References:
- Atri, Mostafa M.D. FRCPC. Ectopic Pregnancy Versus Corpus Luteum Cyst Revisited, Best Doppler Predictors. 2003, 22:1181-1184.
- Blaivas, Michael M.D. Reliability of Adnexal Mass Mobility in Distinguishing Possible Ectopic Pregnancy From Corpus Luteal Cysts. Journal of Ultrasound in Medicine. 2005; 24:599-603.
- Kirk, Emma MBBS. Diagnosis of ectopic pregnancy with Ultrasound. Best Practice & Research Clinical OBGYN. 2009, 23:501-508.
- Lin, Edward P. M.D. Diagnostic Clues to Ectopic Pregnancy. Radiographics 2008. 28:1661-1671.
- Steine, Margorie M.D. Sonographic Comparison of the Tubal Ring of Ectopic Pregnancy With Corpus Luteum. Journal of Ultrasound in Medicine. 2004, 23:57-62
Michael Bazylewicz, MD
Georgetown University Hospital
Washington, DC