Vascular
Clinical history:
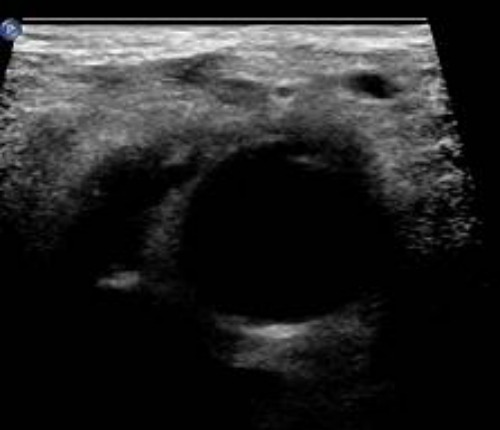
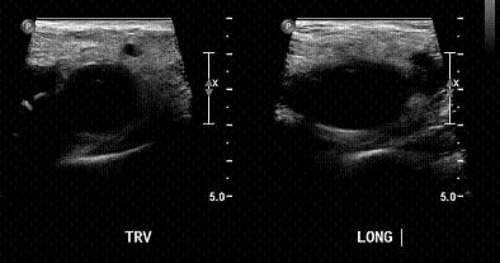
Clinical History: 66 year old female with history of right cerebellar AVM status post angiogram 2 days prior. She has subsequently developed right lower extremity swelling. A lower extremity venous Doppler was negative for DVT; however, the following was seen near the common femoral artery:


Differential considerations include (Choose all that apply):
- Hematoma
- Pseudoaneurysm
- Abscess
What ultrasound technique(s) would be most useful to workup and diagnose this lesion? (Choose all that apply)
- Harmonics
- Color Doppler
- Power Doppler
- Spectral Doppler
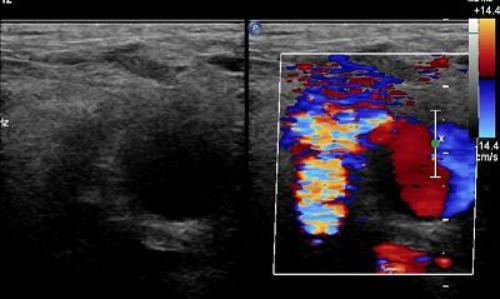
Given the following images, what is the most likely diagnosis:


Name the following sign:

- The turbulent flow sign
- The flowing neck sign
- The to-and-fro sign
- The yin-yang sign
Question 1: A,B,C
Multiple complications can occur after arterial angiography including hematoma, pseudoaneurysm, arteriovenous fistula and arterial occlusion, most of which could cause a degree of swelling. Of these, hematoma is by far the most common.
Question 2: B, D
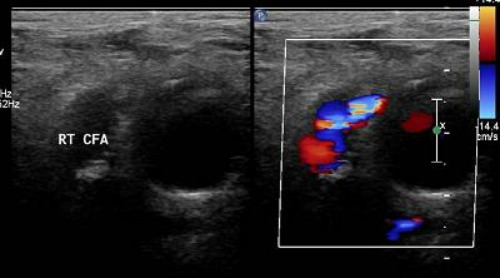
Absence of flow is suggestive of hematoma, while presence of flow is more consistent with pseudoaneurysm. Particularly, turbulent flow in the lesion is highly suggestive of pseudoaneurysm. This lesion is large enough that if present, flow would likely be detected with color Doppler. Other smaller lesions or lesions with slow flow would potentially benefit from power Doppler.
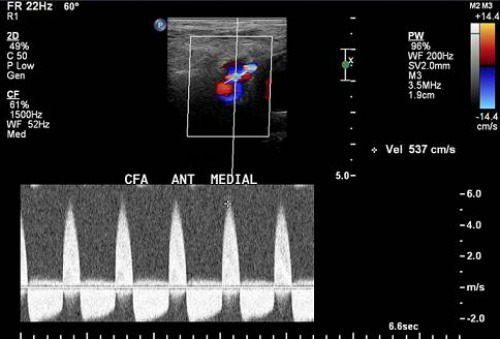
Spectral Doppler will help to demonstrate the pathognomonic “to and fro” flow pattern in the neck of the aneurysm. (See below for further explanation).
Adjusting harmonics and other parameters may help demonstrate the presence of debris with variable echogenicity, indicating repeat bleeding, which is seen more often in a pseudoaneurysm; however, these findings are not pathognomonic and thus cannot be relied upon to differentiate the two entities.
Question 3: Pseudoaneurysm.
There are two main findings which suggest the diagnosis of pseudoaneurysm:
- Neck communicating with the common femoral artery. By definition a pseudoaneurysm communicates with the feeding artery. In contrast a hematoma does not have a “neck.”
- “Yin-Yang” sign – indicates bidirectional flow within the lesion from arterial blood flowing into the lesion, which may resemble its namesake. This sign is less specific and can be seen with other lesions.
Question 4: C
The “to and fro” sign is sited by many to be the most specific sign of a pseudoaneurysm. This is characterized by reversal of flow in the neck during diastole, due to changes in pressure gradients. In systole, the pressure is higher on the arterial end, thus blood flows into the pseudoaneurysm. During diastole, the pressure is now higher in the pseudoaneurysm, due to wall forces in the aneurysm sac secondary to distension and decreased arterial pressure. This phenomenon leads to a cyclical change in flow through the neck between systole and diastole, which results in the above findings.
Key Points:
- Pseudoaneurysms are a relatively uncommon occurrence after femoral access for endovascular procedures, with rates quoted in the literature ranging from 0.1% to 2.2%. This incidence has been increasing in recent years as more patients are on anticoagulants.
- A pseudoaneurysm is a “false” aneurysm and is essentially a communicating hematoma that is not contained by all layers of a vascular structure.
- One often suggested mechanism for pseudoaneurysm formation is puncture below the femoral head, as there is no bony prominence to aid in compression.
- Pseudoaneurysms tend to present as pain, swelling and occasionally a pulsatile mass due to the arterial flow into (and out of) the aneurysm.
- Ultrasound is the imaging study of choice for diagnosis.
- The key ultrasound findings of pseudoaneurysm are: Neck communicating with aneurysm.
- “To and fro” sign – pathognomonic – diastolic flow reversal in aneurysm neck
- Yin-yang/Turbulent flow sign – Turbulent flow in the aneurysm sac, may resemble yin yang
- Complications include: rupture, compression of other vessels leading to ischemia, infectious and thromboembolic source.
Treatment options include:
- Ultrasound guided compression repair
- Involves periods of compression of the aneurysm neck with ultrasound with goal of stopping flow.
- Time consuming
- High rate of recurrence (up to 35% in patients on anticoagulants)
- Percutaneous treatment
- Thrombin
- Most commonly used treatment
- Coils
- Placed in neck or sac
- Covered stent
- Excludes the pseudoaneurysm
- Surgical ligation
- Reserved for emergent situations, such as limb ischemia or rupture
- Also used in cases of treatment failure
Sources:
- Abu-Yousef, M, et al. The “To-and-fro” Sign: Duplex Doppler Evidence of Femoral Artery Pseudoaneurysm. AJR 1988. 150:632-634.
- Altin, R, et al. Pseudoaneurysm and Arteriovenous Fistual After Femoral Artery Catheterization: Association with Low Femoral Puncture. AJR 1989. 152 (3):629-631.
- Lenartova, M, et al. Iatrogenic Pseudoaneurysm of Femoral Artery: Case Report and Literature Review. CM&R 2003:1, Number 3: 243-247.
- Rozen, G, et al. The To and Fro Sign: The Hallmark of Pseudoaneurysm. IMAJ 2001;3: 781-782.
Nicholas Caruana, MD
Georgetown University Hospital
Washington, DC